ICU bed no 2
E.RISHITHA REDDY
ROLL.NO-30
“This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent.
Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs.
This E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment box is welcome."
I've been given this case, in an attempt to understand the topic of "patient clinical data analysis" and to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations as well as to come up with a diagnosis and treatment plan.
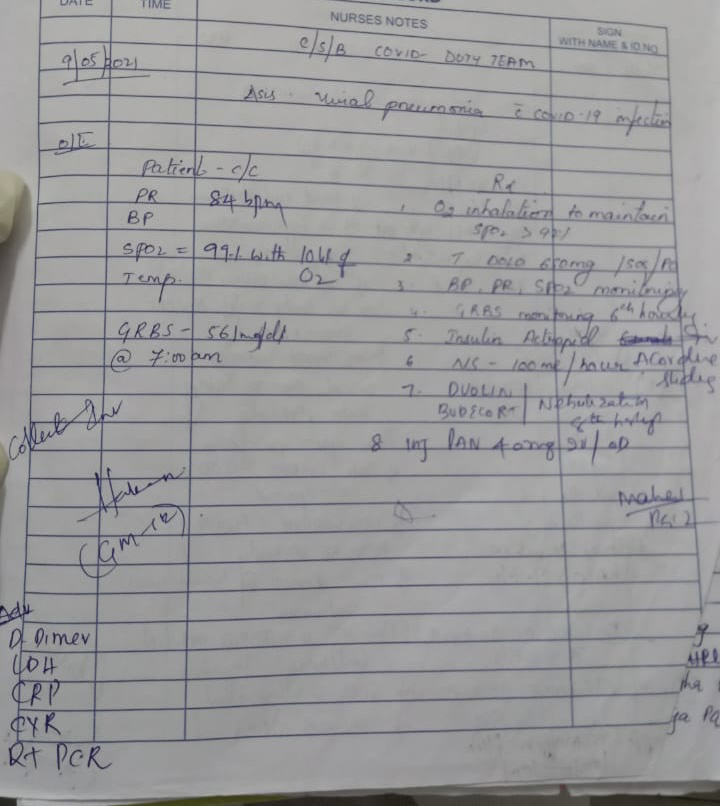
CASE REPORT-
A 67 yr old female came to the casualty with c/o altered sensorium since 2 pm ( 7/9/21)
History of present illness :
Patient was apparently asymptotic before 2 pm (7/9/21) , then she developed altered sensorium sudden in onset .
She had repeated episodes of fainting from past 6 months with a duration episode of 15 min and after regaining consciousness she couldn’t recognise any thing for few min and then become normal after that.
H/o seizures on/off since 10 yrs
Patient was normal 6 months back then developed-loss of speech with altered sensorium.
Past history:
MRI : 6 months back
Multiple calcified granulomas ( largest measuring 1.0X0.8 cm in the frontal lobe )
Chronic laccunar infarcts in pons -on Left side ,B/L basal ganglia
Small vessels ischaemic changes
Past history:
No h/o HTN , DM, CAD and any other chronic illness
Personal history:
Appetite:N
Diet :veg
Sleep :regular
B/B: regular /normal
No addictions
Family history:
Not significant.
Physical examination:
PICKLE : - ve
Temp ; afebrile
PR: 98bpm
RR: 22
BP :140/90 mmhg
Spo2 : 98
GRBS :209 mg%
Systemic examination:
CVS : s1 s2 +
Respiratory: BAE+,NVBS
Abdomen : soft , non tender
CNS : unconscious
Speech : aphasic
No signs of meningeal irritation
Tone :
Right U/L: increased , L/L- normal
Left U/L: increased , L/L- normal
GCS: E1V1M1
Reflexes : knee , ankle - absent
Investigation reports:
Blood urea-

Serum Creatinine-

Utica acid serum-

Serum electrolytes-

Liver function tests-

ECG-


Provisional diagnosis:
Altered sensorium under evaluation


Comments
Post a Comment